For me yes. Worse lipids on a lower dose of primo than a higher dose of tren.Is primo one of the worst offenders when it comes to lipids?
MESO-Rx
Anabolic Steroids
Navigation
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
More options
Style variation
Guest viewing limit reached
- You have reached the maximum number of guest views allowed
- Please register below to remove this limitation
- Already a member? Click here to login
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Had a Heart Attack today at age ~30. Be safe guys.
- Thread starter ChemBB
- Start date
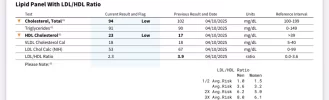
Kind of scary that your lipids lol that good but you just had a heart attack.Got bloods yesterday, some updates:
GEAR:
- 300 Test
- 8 Reta + 2 Sema
- 4iu GH
- 20 Cialis
- 10 Cardarine
LIPIDS:
View attachment 352116
KIDNEYS:
View attachment 352117
LIVER:
View attachment 352118
METABOLIC:
View attachment 352119
dinfar1337
Member
its very easy to make those models with simple tools in word. we play with it from elementary school here in eu.It looks like a pharmacy printout of some kind which was why I'm asking
3d and adding lines / shapes and sizing as you want.
you could also just steal some "3d sketch drawing round pill" or whatever shape you want and use Remove Background from Image for Free – remove.bg
dinfar1337
Member
.webp")
something like this could look nice
ChemBB
Member
I stopped using AI about 5 years ago and will never use them againDo you use an Ai with that dose?
Ah, that's from hospital mate!How are you getting this printout?
I do mine in Excel but this looks way cooler
I don't think so, but maybe I'm mistaken?Is primo one of the worst offenders when it comes to lipids?
They did a 1968 study giving female breast cancer patients 1,200mg Primo / wk and that wasn't one of the acute sides mentioned
Attachments
What does your estrogen hover around when. You did 350 for that periodI stopped using AI about 5 years ago and will never use them again
Ah, that's from hospital mate!
I don't think so, but maybe I'm mistaken?
They did a 1968 study giving female breast cancer patients 1,200mg Primo / wk and that wasn't one of the acute sides mentioned
ChemBB
Member
At 300-350 Test by itself, E2 = ~40-90 generallyWhat does your estrogen hover around when. You did 350 for that period
When I did 250 Test + 200 Mast E for 8 months back in 2017, my E2 was 19

No sides with it getting up to 90?At 300-350 Test by itself, E2 = ~40-90 generally
When I did 250 Test + 200 Mast E for 8 months back in 2017, my E2 was 19
View attachment 352241
Also how was your HDL on the 19 bloofwork? When I run test and primo (even a baby dose of prim) it lowers my estrogen so much it ruins my lipids.
ChemBB
Member
No sides with it getting up to 90?
No sides as far as I can tell -- I have gyno from when I was 17 and first started gear. (I kept upping Dbol dose until I was taking 100mg a day because I wasn't sure if it was "doing anything". </facepalm>)
So if my E2 gets too high, I can feel my nips burning + gyno growing, which I don't.
I have libido issues but it's been that way forever regardless of what I take. Pretty sure it's from years of drug addiction messing up my neurochemistry.
I wish I could tell you. I didn't check my lipids EVER when I was young, only started in the last few years =(Also how was your HDL on the 19 bloofwork?
I am sorry for you but you didn't write anything about your lifestyle.Well, it finally happened to me.
Near end of my workout today I start feeling chest tightness & pain, hard to breathe.
Go to emergency room, get told I'm having a heart attack (STEMi).
"A 99% subtotal blockage was found in the second obtuse marginal (OM2) branch of left circumflex (LCx) artery."
Likely from vulnerable plaque rupturing during the workout and the thrombosis that follows narrowing the artery.
Single-vessel disease, no other obstructive disease discovered during angiogram.
Code:- Impression: Inferior ST elevation microinfarction with culprit lesion of second obtuse marginal 99 percent subtotal occlusion - Successful imaging guided primary PCI of second obtuse marginal with 3 x 20 mm Synergy stent - Normal LVEDP - No aortic stenosis - Recommendation - Start aspirin 81 mg daily for lifelong - Start Brilinta 90 mg twice a day for at least one year - Start high intensity statin therapy for goal of less than 55 - Obtain echocardiogram - Cardiac rehabilitation referral
Summary of Echocardiogram w/ contrast performed afterwards:
Code:- Mildly dilated left ventricle - Moderate concentric LV hypertrophy - Mildly reduced LV systolic function - EF 45–50% (down from 55% post-op, plausible post-MI myocardial "stunning", expect recovery) - Hypokinesis of inferoposterior wall - Mild to moderately enlarged left atrium - Mild to moderate mitral regurgitation - Mild tricuspid regurgitation - Mild pulmonic regurgitation
Stay safe, folks.
Maybe you run with high BP since a long time, maybe you eat tons of saturated fats.
Stay safe doesn't mean anything.
Banana Joe
Member
Were you then sure it "does something" when you had hit 100mg?No sides as far as I can tell -- I have gyno from when I was 17 and first started gear. (I kept upping Dbol dose until I was taking 100mg a day because I wasn't sure if it was "doing anything". </facepalm>)
Those were the golden years for anabolics. They used them to treat anything. No matter what illness you had, doctors gave you a chance to get swole.They did a 1968 study giving female breast cancer patients 1,200mg Primo / wk and that wasn't one of the acute sides mentioned
I wish that had never changed. Just imagine what kind of steroids we would have by now, had they poured GLP1-drug kind of money into researching them.
Last edited:
ChemBB
Member
Were you then sure it "does something" when you had hit 100mg?
Yeah, because I got gyno almost instantly LMAO
Went from no sides, not sure if it was fake sugar powder, to suddenly I wake up and my nips burning, hurting and itching
That's when I realized it was definitely dbol.
I wish that had never changed. Just imagine what kind of steroids we would have by now, had they poured GLP1-drug kind of money into researching them.
I didn't want to be sad this early in the morning.... =(
OldGHGuy
Member
Received my bloods back this week and have some relavant results attached. Running 250 Test, 150 Primo, 2.4 GH, 5 mg Tirz. A few interesting points including improvements from previous when running just 140 Test TRT. 40mg Atorvastatin year round.A genuine negative for calcification, but plaque, unless you've had sub 60 LDL your entire life, you have some degree of accumulation. During the Korean War the US started checking soldiers during autopsies, and for example, 85% of 22 year olds had established plaque, some even had arteriosclerosis!
Within a generation or two this disease will be extinct. You'll get a lifetime PCSK9 inhibitor, essentially a heart disease "vaccination" during childhood that'll neutralize PCSK9 for good and there won't be any accumulation of plaque.
I did find out this is too much Primo for this level of Test for me as my sensitive E2 came back at 16. Strangely no joint issues but stomach bloating that I believe I wrongly attributed to a virus but now believe it was the low E2
Attachments
Last edited:
Banana Joe
Member
And there was me, when I was even a few years older, keeping my 2x5mg Dbol run to 5 weeks, because I was worried about my liver. When the general forum consensus was that 8 weeks are a safe length for such a cycle, obviously at higher doses than mine.Yeah, because I got gyno almost instantly LMAO
I haven't given up that there will not be an anabolic renaissance.I didn't want to be sad this early in the morning.... =(
Just imagine cheap gene testing and AI designing afforable custom anabolics for every man.
PS: Thanks again for putting this all out there! There will be that one guy, that you will never know about, that you scared into being more more diligent with his health.
Ghoul
Member
Received my bloods back this week and have some relavant results attached. Running 250 Test, 150 Primo, 2.4 GH, 5 mg Tirz. A few interesting points including improvements from previous when running just 140 Test TRT. 40mg Atorvastatin year round.
I did find out this is too much Primo for this level of Test for me as my sensitive E2 came back at 16. Strangely no joint issues but stomach bloating that I believe I wrongly attributed to a virus but now believe it was the low E2
Not bad man!
If you switch to Pitavastatin, you may see a 10+ point boost to HDL, a very clinically significant increase that would make plaque regression move at a good pace with your fairly low LDL. I saw an 11 point jump from 39 to 51 on 200mg Test. Unless you're on Atorvastatin due to kidney disease, Pita is superior.
If anyone needs inspiration, my lipids from September 2024:

To September 2025:

This is with Pitavastatin 4, Ezetimebe, and Repatha. The Repatha is only adding 10-12% more improvement to the other two though.
After these, and stress echo + CPET results were sent, my preventative cardiologist added a note:
"You have undergone a complete cardiometabolic risk inversion. From a 10-year ASCVD risk near 18%, you now present with optimal blood pressure, an LDL profile in the lowest 0.1% of the population, and endurance-level aerobic fitness. Your current risk is...
To September 2025:
This is with Pitavastatin 4, Ezetimebe, and Repatha. The Repatha is only adding 10-12% more improvement to the other two though.
After these, and stress echo + CPET results were sent, my preventative cardiologist added a note:
"You have undergone a complete cardiometabolic risk inversion. From a 10-year ASCVD risk near 18%, you now present with optimal blood pressure, an LDL profile in the lowest 0.1% of the population, and endurance-level aerobic fitness. Your current risk is...


sionnach
New Member
I'm sure you've mentioned this in one of your many posts, but what HDL-promoting supps do you take personally (fish/krill oil, omega 3, dietary sources, niacinamide etc)?Not bad man!
If you switch to Pitavastatin, you may see a 10+ point boost to HDL, a very clinically significant increase that would make plaque regression move at a good pace with your fairly low LDL. I saw an 11 point jump from 39 to 51 on 200mg Test. Unless you're on Atorvastatin due to kidney disease, Pita is superior.
If anyone needs inspiration, my lipids from September 2024:
To September 2025:
This is with Pitavastatin 4, Ezetimebe, and Repatha. The Repatha is only adding 10-12% more improvement to the other two though.
After these, and stress echo + CPET results were sent, my preventative cardiologist added a note:
"You have undergone a complete cardiometabolic risk inversion. From a 10-year ASCVD risk near 18%, you now present with optimal blood pressure, an LDL profile in the lowest 0.1% of the population, and endurance-level aerobic fitness. Your current risk is...
dinfar1337
Member
your september cholesterol is my goal man.Not bad man!
If you switch to Pitavastatin, you may see a 10+ point boost to HDL, a very clinically significant increase that would make plaque regression move at a good pace with your fairly low LDL. I saw an 11 point jump from 39 to 51 on 200mg Test. Unless you're on Atorvastatin due to kidney disease, Pita is superior.
If anyone needs inspiration, my lipids from September 2024:
To September 2025:
This is with Pitavastatin 4, Ezetimebe, and Repatha. The Repatha is only adding 10-12% more improvement to the other two though.
After these, and stress echo + CPET results were sent, my preventative cardiologist added a note:
"You have undergone a complete cardiometabolic risk inversion. From a 10-year ASCVD risk near 18%, you now present with optimal blood pressure, an LDL profile in the lowest 0.1% of the population, and endurance-level aerobic fitness. Your current risk is...
im not on statins yet but with reta/cardio im on 45 hdl 60 ldl. trying to squeeze last bit of hdl up and ldl down before jumping on.
OldGHGuy
Member
Thanks brother. I will give Pita a try as moving the needle on HDL has been really tough. BTW - I bought some Ezitimebe on your recommendation but after these bloods I'm wondering if I need it? Thoughts?Not bad man!
If you switch to Pitavastatin, you may see a 10+ point boost to HDL, a very clinically significant increase that would make plaque regression move at a good pace with your fairly low LDL. I saw an 11 point jump from 39 to 51 on 200mg Test. Unless you're on Atorvastatin due to kidney disease, Pita is superior.
If anyone needs inspiration, my lipids from September 2024:
To September 2025:
This is with Pitavastatin 4, Ezetimebe, and Repatha. The Repatha is only adding 10-12% more improvement to the other two though.
After these, and stress echo + CPET results were sent, my preventative cardiologist added a note:
"You have undergone a complete cardiometabolic risk inversion. From a 10-year ASCVD risk near 18%, you now present with optimal blood pressure, an LDL profile in the lowest 0.1% of the population, and endurance-level aerobic fitness. Your current risk is...
Ghoul
Member
Thanks brother. I will give Pita a try as moving the needle on HDL has been really tough. BTW - I bought some Ezitimebe on your recommendation but after these bloods I'm wondering if I need it? Thoughts?
Ezetimibe is the most benign LDL reducing compound there is. Since it's "cost free", and there's a measurable benefit to getting LDL below 40 per the latest guidelines, I strongly recommend you use it. You're in or near plaque regression territory. Studies show lower LDL is the primary driver of regression. The sooner and faster regression takes place the "deeper" the cleaning of your arteries will be. The longer plaque remains the greater the amount that will harden and become unremovable,
The LDL drop from Ezetimebe isn't usually huge, but if you happen to be in the 15% of genetic "dietary cholesterol hyperabsorbers", it may be a very large reduction.
Ghoul
Member
I'm sure you've mentioned this in one of your many posts, but what HDL-promoting supps do you take personally (fish/krill oil, omega 3, dietary sources, niacinamide etc)?
None. The latest ESC (Euro Society of Cardiology) lipid guidelines directly addressed this. The problem with HDL increases from supplements is that they don't increase production of APO-I. This is the protein that gives HDL its ability to remove cholesterol from arteries and transport it back to the liver. So what's happening is you're producing low or non-functional HDL. At best it's neutral, but giving a deceptive sense of being useful based on the HDL number, At worst, there's evidence non functional HDL becomes inflammatory.
Pitavastatin stimulates the production of APO-I, along with HDL. So Pitavastatin is producing functional HDL. In fact the boost to APO-I is likely improving the function of all your HDL.
The only other way to significantly increase APO-I is exercise.
After LDL, HDL function (efflux capacity), is the greatest factor determining how much regression of plaque is possible.
The reason for the "rush" is that once LDL is low enough that you're no longer depositing it in arteries, there's a limited window for regression before plaque stabilizes, which is good, but means it's no longer able to be removed. Removal is better than stabilization.
You can get it tested with Boston Heart Diagnostics HDL Map test if you're curious, $169.

A new way of looking at ‘good’ cholesterol | Heart | UT Southwestern Medical Center
Knowing how your cholesterol functions can help doctors determine your heart disease risk. A UT Southwestern cardiologist uses a garbage truck analogy to explain “cholesterol efflux.”


Last edited:
Similar threads
- Replies
- 0
- Views
- 2K